Troubleshooting Finger Deviation with the SaeboFlexUpdated 4 months ago
While in the SaeboFlex, clients with hypertonicity and/or soft tissue shortening can exhibit finger deviation during grasping.
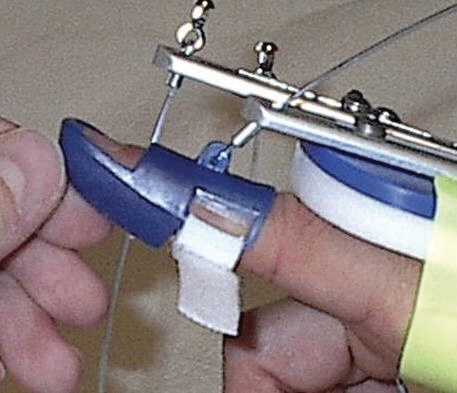
Finger deviation can occur in a radial or ulnar direction. The below is an example of the long finger deviating in a radial direction. Although, the deviation appears to be occurring at the PIP joint of the 3rd digit, however, the proximal phalanx is actually “rotating” at the MCP joint causing the deviation. The goal will be to eliminate or reduce the rotation or “spinning” of the respective MCP joint.
 |  |
This rotation can be the result of a number of issues, which include:
• MCP joint laxity
• Weakness of the intrinsic muscles of the hand
• Soft-tissue shortening and/or hypertonicity
• Fatigue
Did you know? If deviation is not seen initially, but occurs after the client has been grasping & releasing for several repetitions, then fatigue is often the cause.
Strategies to Consider:
Since deviation is a result of rotation of the proximal phalanx at the MCP joint, the first step is to ensure optimum stability.
1. Position the Dorsal Hand Piece as close as possible to the PIP joint of the 3rd digit, but without covering the PIP joint of the 2nd or 5th digit.
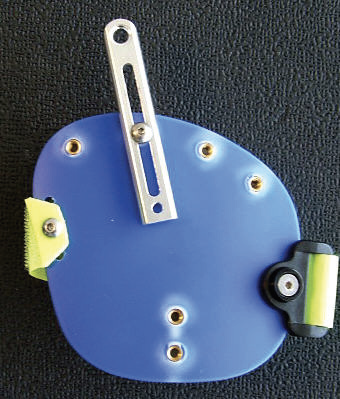
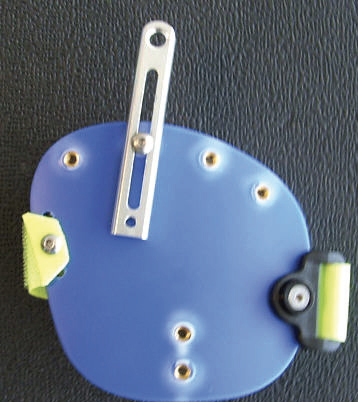
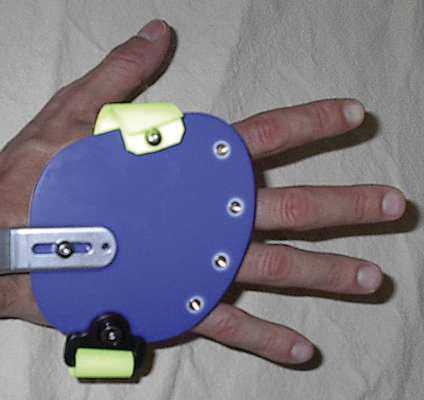 Dorsal Hand Piece position for mild to moderate tone. Dorsal Hand Piece position for mild to moderate tone. | 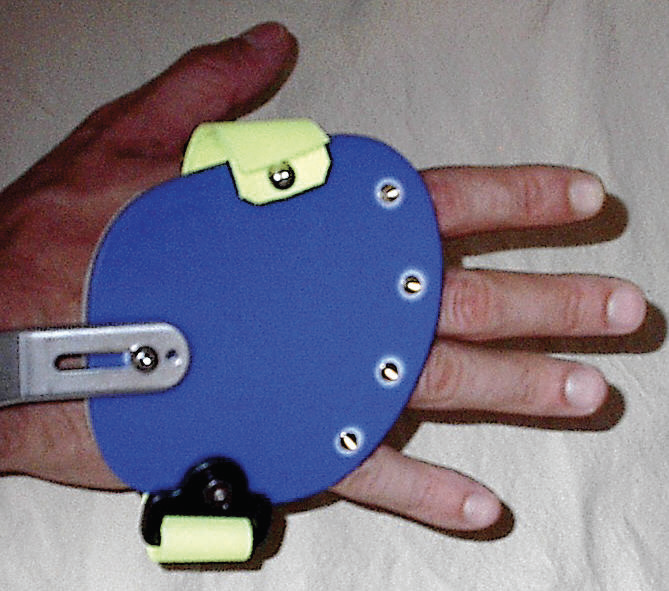 Dorsal Hand Piece position for severe tone. Dorsal Hand Piece position for severe tone. |
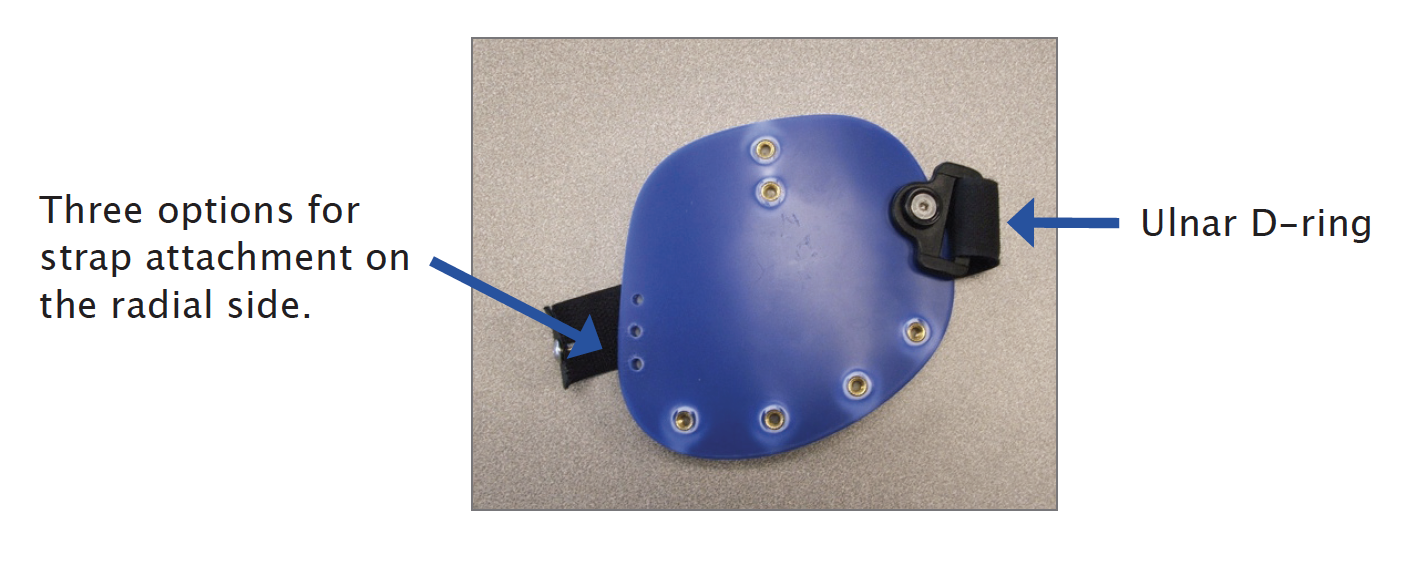
2. Make sure the Dorsal Hand Strap is snug and positioned on the volar surface of the metacarpal heads.

Note: The Dorsal Hand Strap can be positioned more proximal or distal by moving the strap on the radial side to one of the three pre-drilled holes.
3. Position the Finger Lead Mounts closer to a 90° angle of pull (but not greater) as this will provide more control distally. If the angle is greater than 90°, the Digit Cap will migrate off the tip of the finger.
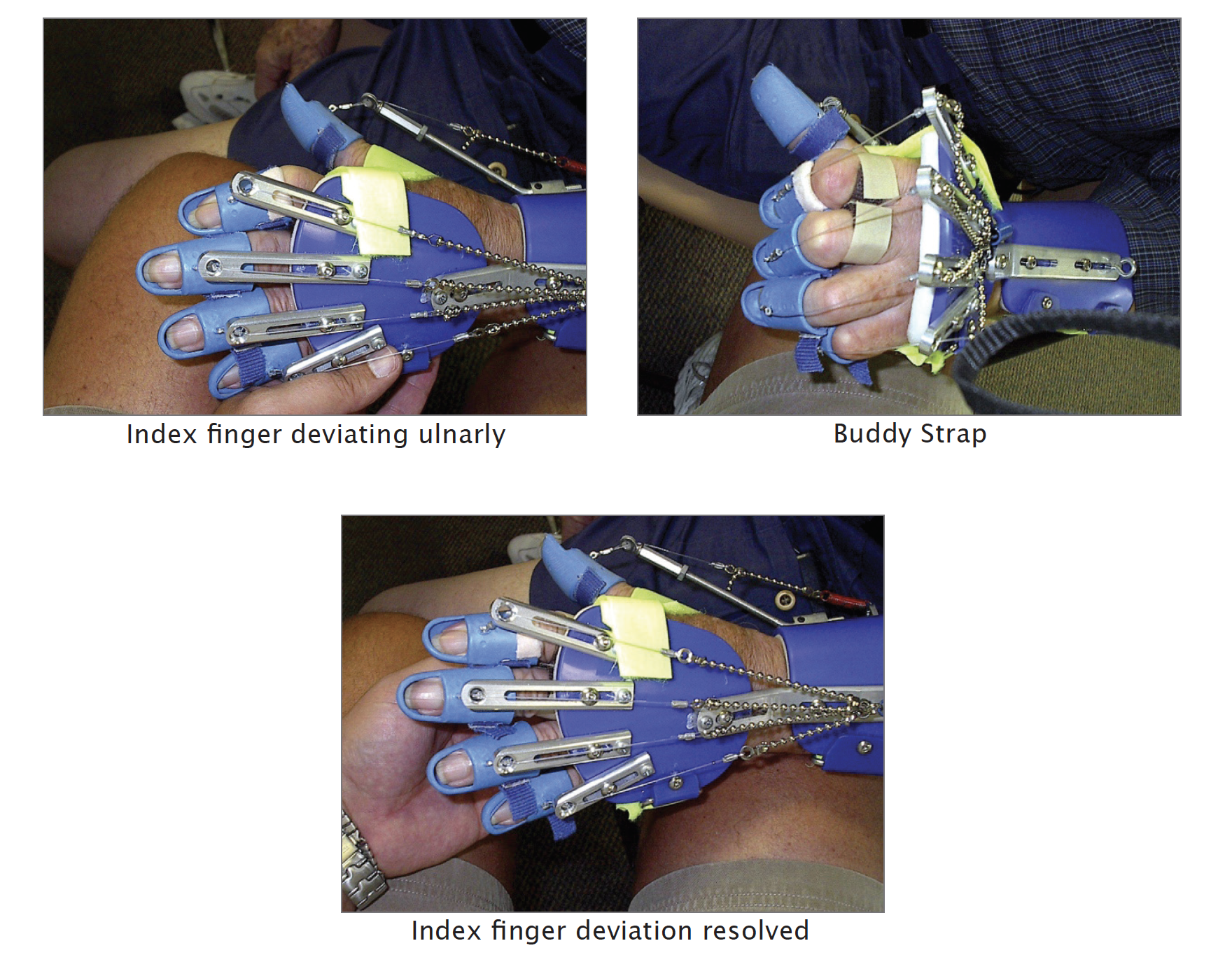
4. Splay the Finger Lead Mounts in the opposite direction of the deviation. Loosen the screw on the Finger Lead Mount and splay ulnarly to reduce radial deviation and radially to reduce ulnar deviation.
 |  |
5. Apply a Buddy Strap to “pull” the proximal phalanx back under the dorsal hand piece if the index finger is deviating ulnarly (toward the palm of the hand), or if the little finger is deviating radially (toward the palm of the hand).
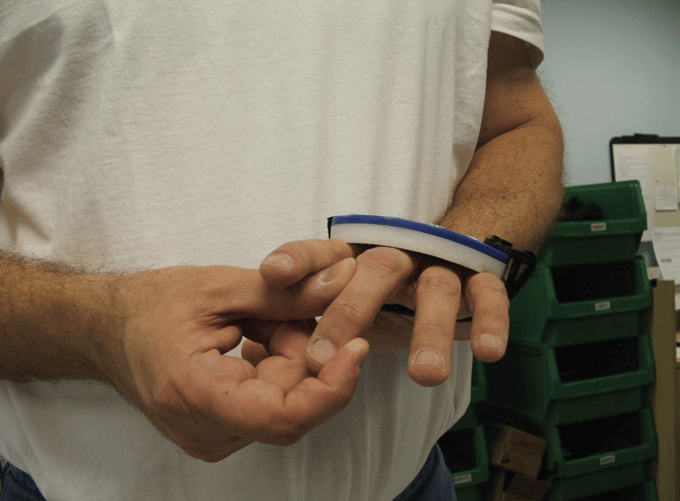
6. Place a piece of blue foam tubing, used to build up handles, over the proximal phalanges of the digits that are deviating. Simply cut enough of the foam tubing to cover the proximal phalanx. Make sure that the foam does not block the PIP joint. This will provide support for the MCP joints limiting the amount of rotation that occurs. If this does not work, try placing an additional foam ring on the adjacent digit.
 |  |
7. Apply a bi-pull technique (2 lines of pull) to the deviating finger(s). This allows you to use a second line on the same finger to “pull” the digit in the opposite direction of the deviation.
8. Change from a 35° wrist mount to a 15° degree wrist mount. By lowering the wrist angle, the degree of stretch provided on the long finger flexors will reduce, therefore, minimizing the amount of deviation at the digits.
Important: It is recommended that you try to resolve the issue by performing the bi-pull technique first before considering a lower wrist mount angle. By keeping the wrist mount at 35°, this will maintain the optimum stretch on the long finger flexors during repetitive grasp and release which may help reduce hypertonicity.